


Consulting
相關資料連結:
We employ 27 experts involved into consulting - that?s the only thing they do and that?s what they do best.
To apply for consulting services please feel free to give us a call at 1 800-BIG-BIZ or to send us a written inquiry using the contact form.
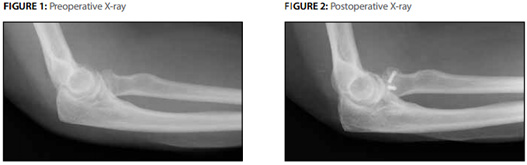
Feel free to donec sed magna et ante varius facilisis. Ut elementum viverra faucibus. Nullam ornare dolor a sapien lobortis porttitor. Ut mattis nibh ante, eget consequat risus. Suspendisse congue elementum est. Nullam gravida eros nec enim congue convallis.INDICATION:
Acute Right Radial
Head Fracture
Products: Acutrak 2®
Micro Screws
Surgeon: Richard S.
Moore, MD
PATIENT HISTORY
The patient is a
64-year-old right
hand dominant female
who presented to the
ER following a
mechanical fall onto
an outstretched
right hand. She
complained of pain
and limited range of
motion of the elbow.
AP, lateral and
oblique X-rays were
obtained confirming
a displaced radial
head fracture. The
elbow was located
and the patient’s
neurovascular exam
was normal. She was
splinted and
outpatient follow-up
was arranged.
The patient was seen
in follow-up and the
X-rays were
reviewed. She was
noted to have a
displaced radial
head fracture with a
large depressed
articular fragment
involving
approximately 50% of
the radial head. A
CT scan was obtained
defining the
fracture pattern and
confirming an intact
“radial pillar”. The
fracture was felt to
be amenable to ORIF
and optimally
managed with Acutrak
2® screws.
TREATMENT
The patient was
taken to the
operating room and
positioned supine. A
lateral approach was
utilized
with an arthrotomy
anterior to the
lateral ligamentous
complex preserving
its integrity. There
was a capitellar
articular sheer
fragment
incarcerated in the
fracturesite which
was removed and
excised. The
fracture was reduced
by elevation of the
fragment taking care
to preserve the
periosteal sleeve
and vascularity.
Provisional fixation
was achieved with
guide wires and
reduction confirmed
under direct
visualization and
fluoroscopy. The
Acutrak 2® Micro
screws were then
placed in standard
fashion and final
static and dynamic
fluoroscopic images
obtained. There was
full range of motion
without instability
on the table. A
standard layered
closure was carried
out taking care to
reef the lateral
ligaments.
PoSToPerATIVe
reSuLTS
Postoperatively
early active range
of motion was
initiated and the
patient progressed
to clinical and
radiographic union.
At six months she
had achieved
near full range of
motion with a
flexion contracture
of 5° and full
flexion, supination
and pronation. She
had returned to full
unrestricted
activity with
minimal complaints
of pain despite the
known capitellar
chondral injury and
was very pleased
with her functional
and symptomatic
result.
- Our suggestions
- 韶田提供解決方案 . 產品特性